Part D. Chapter 6: Cross-Cutting Topics of Public Health Importance
What is the relationship between the intake of low-calorie sweeteners (LCS) and risk of type 2 diabetes?
Conclusion Statement: Long-term observational studies conducted in adults provide inconsistent evidence of an association between LCS and risk of type 2 diabetes.
DGAC Grade: Limited
Review of Evidence
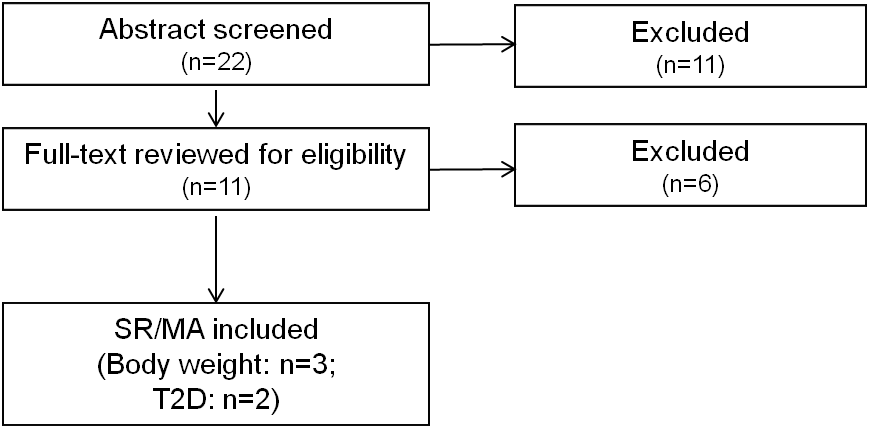
Evidence to address the impact of LCSs (specifically artificially sweetened soft drinks, ASSD) on risk of type 2 diabetes comes from two SRs/MA published between January 2010 and August 2014.1 2 The data from one of the reviews also is represented in the second review.
Greenwood et al. reported that higher consumption of ASSD predicts increased risk of type 2 diabetes.1 The summary RR for ASSD on type 2 diabetes risk was 1.13 (95% CI = 1.02 to 1.25, p<0.02) per 330 ml/day, based on four analyses from three prospective observational studies. Although the finding indicates a positive association between ASSD and type 2 diabetes risk, the trend was not consistent and may indicate an alternative explanation, such as confounding by lifestyle factors or reverse causality (e.g., individuals with higher BMI at baseline may use ASSD as a means to control weight).
Romaguera et al. also reported that higher consumption of ASSD was associated with increased risk of type 2 diabetes.2 In adjusted models, one 336 g (12 oz) daily increment in ASSD consumption was associated with a hazard ratio for type 2 diabetes of 1.52 (95% CI = 1.26 to 1.83). High consumers of ASSD showed almost twice the hazard ratio of developing type 2 diabetes compared with low consumers (adjusted HR = 1.93; 95% CI = 1.47 to 2.54; p for trend <0.0001). However, the association was attenuated and became statistically not significant when BMI was included in the model (HR = 1.13, 95% CI = 0.85 to 1.52; p for trend = 0.24). The authors offered these interpretations of the findings: “In light of these findings, we have two possible explanations of the association between artificially sweetened soft drinks and diabetes: (1) the observed association is driven by reverse causality and residual confounding, given that the underlying health of people consuming artificially sweetened soft drinks may be compromised and their risk of type 2 diabetes increased; or (2) the association between artificially sweetened soft drinks and type 2 diabetes is mediated through increased BMI.” The authors argued that explanation 1 is more likely correct based on reverse causality, but new research would be needed to clarify the issue.
Collectively, both studies report a positive association between ASSD and type 2 diabetes risk that was confounded by baseline BMI. The experimental designs of the studies included in these reviews analyzed associations, but precluded the assessment of cause and effect relationships, and future experimental studies should examine the relationship between ASSD and biomarkers of insulin resistance and other diabetes biomarkers.
Table 1. Summary of existing reports, systematic reviews, and meta-analyses examining the relationship between the intake of low-calorie sweeteners (LCS) and risk of type 2 diabetes
|
Author, Year
Publication Type
AMSTAR Rating* |
Low-calorie sweeteners (LCS) Definition
Outcomes Considered |
Date Range Searched
Criteria Used |
Included Studies (Number and Design)
|
Recommendations, Evidence/Conclusion Statements, and/or Main Results from Existing Report/ SR/ MA |
|---|---|---|---|---|
|
Greenwood, 2014
Systematic Review and Meta-Analysis
AMSTAR: 8/11 |
Carbonated artificially sweetened soft drinks (ASSD)
Converted consumption to ml/d to explore linear & non-linear dose-response trends
Incidence of T2D |
1990 to Nov 2009, with an update in June 2013 PCSs; English language; original research article; at least 3 yr duration; differentiated between sugar and artificially sweetened beverages; participants from a generally healthy population |
3 publications on 4 cohorts examined association of artificially sweetened soft drink (ASSD) intake and T2D risk.
A pooled estimate of RR from linear dose-response meta-analysis was also produced. |
Conclusion: ASSD conclusion: Included studies were observational, thus results should be interpreted cautiously. Meta-analyses demonstrate positive association of ASSD intake and T2D risk. Association was stronger and more consistent for sugar-sweetened beverages than for ASSD and together with the effect of adjusting for BMI (attenuation), may indicate an alternative explanation for observed association such as lifestyle or reverse causality.
Main Results: ASSD pooled estimate of relative risk from linear dose-response meta-analysis was 1.13 (95% CI: 1.02 to 1.25)/330 ml ASSD (p=0.02). Substantial heterogeneity between cohort studies (I2=87%); few studies available to explore sources of heterogeneity. Some evidence of mild nonlinearity in the dose-response curve; number of included studies was small
|
|
Romaguera, 2013 (Note: Included in Greenwood, 2014)
Meta-Analysis of eight cohorts from the EPIC study
AMSTAR: N/A |
Artificially sweetened soft drink (ASSD)
Incidence of T2D |
N/A Excluded those with evidence of T2D and those within the lowest and highest 1% of the cohort distribution of the ratio of reported total energy intake: energy requirement and those with missing information on diet, physical activity, level of education, smoking status, or BMI |
Eight cohorts of the EPIC study |
Conclusion: Study reported association between ASSD and T2D that disappears when models are adjusted for baseline BMI. Main Results: High consumers of ASSD showed almost twice the hazard ratio (HR) of developing T2D compared with low consumers (adjusted HR 1.93, 95% CI: 1.47 to 2.54; p for trend < 0.0001); association was attenuated and became statistically not significant when BMI was included in the model (HR 1.13, 95% CI: 0.85 to 1.52; p for trend 0.24). Adjusted HR of T2D associated with 12 oz. increment in consumption of ASSD was 1.52 (95% CI: 1.26 to 1.83), which was attenuated and not significant after adjustment for body adiposity measurement. Significant interaction (p=0.03) between consumption of ASSD and BMI category on T2D incidence. In stratified analyses, ASSD consumption was sig. assoc. with T2D incidence in normal weight subjects and was unchanged with adjustment for BMI: HR: 1.43, 95% CI: 1.05 to 1.95). Borderline significance among overweight; no association among obese. |
* A measurement tool for the ‘assessment of multiple systematic reviews’ (AMSTAR)
References Included in the Review
- Greenwood DC, Threapleton DE, Evans CE, Cleghorn CL, Nykjaer C, Woodhead C, et al. Association between sugar-sweetened and artificially sweetened soft drinks and type 2 diabetes: systematic review and dose-response meta-analysis of prospective studies. Br J Nutr. 2014:1-10. PMID: 24932880. http://www.ncbi.nlm.nih.gov/pubmed/24932880
- Romaguera D, Norat T, Wark PA, Vergnaud AC, Schulze MB, van Woudenbergh GJ, et al. Consumption of sweet beverages and type 2 diabetes incidence in European adults: results from EPIC-InterAct. Diabetologia. 2013;56(7):1520-30. PMID: 23620057. http://www.ncbi.nlm.nih.gov/pubmed/23620057
Supplementary Information:
(Note: One search for low-calorie sweeteners and body weight, type 2 diabetes, cardiovascular disease, and dental caries was conducted. Only reviews on body weight and type 2 diabetes were identified and are presented below.)
Methodology
This question was answered using existing SRs/MA published from January 2010 to August 2014.
Search Strategy for Existing Systematic Reviews/Meta-Analyses
PubMed:
(Non-caloric sweeten* OR non caloric sweeten* OR "Non-Nutritive Sweeteners"[Mesh] OR Non-Nutritive Sweetener*[tiab] OR Non Nutritive Sweetener*[tiab] OR low calorie sweeten* OR (artificial* sweeten*) OR “sugar free” OR sugar-free OR saccharin OR aspartame OR acetosulfame OR sucralose OR trichlorosucrose OR neotame OR erythritol OR rebaudioside* OR rebiana OR diet soda* OR diet drink* OR (intense* sweeten*[tiab]))
pooled analysis* OR systematic[sb] OR systematic review* OR meta-analys* OR meta analys* OR lim to SR/MA
Embase:
(Non-caloric NEXT/1 sweeten*) OR (“non caloric” NEXT/1 sweeten*) OR (Non-Nutritive NEXT/1 Sweeten*) OR “Non-Nutritive” NEXT/1 Sweeten* OR “Non Nutritive” NEXT/1 Sweeten* OR “low calorie” NEXT/1 sweeten* OR (artificial* NEXT/1 sweeten*) OR “sugar free” OR sugar-free OR saccharin OR aspartame OR acetosulfame OR sucralose OR trichlorosucrose OR neotame OR erythritol OR rebaudioside* OR rebiana OR diet soda* OR diet drink* OR (intense* NEXT/1 sweeten*) OR advantame OR (sugar NEXT/1 substitute*) OR stevia OR cyclamate* OR (monk NEXT/1 fruit*)
'systematic review'/exp OR 'meta analysis'/exp OR pooled NEXT/1 analysis* OR “systematic review” OR meta NEXT/1 analys*
Cochrane:
(Non-caloric NEXT/1 sweeten*) OR (“non caloric” NEXT/1 sweeten*) OR (Non-Nutritive NEXT/1 Sweeten*) OR “Non-Nutritive” NEXT/1 Sweeten* OR “Non Nutritive” NEXT/1 Sweeten* OR “low calorie” NEXT/1 sweeten* OR (artificial* NEXT/1 sweeten*) OR “sugar free” OR sugar-free OR saccharin OR aspartame OR acetosulfame OR sucralose OR trichlorosucrose OR neotame OR erythritol OR rebaudioside* OR rebiana OR diet soda* OR diet drink* OR (intense* NEXT/1 sweeten*) OR advantame OR (sugar NEXT/1 substitute*) OR stevia OR cyclamate* OR (monk NEXT/1 fruit*)
Inclusion Criteria
Date Range:
- Published between January 2010 and August 2014 (in English in a peer-reviewed journal)
Study Design:
- Systematic review and/or meta-analysis that included randomized controlled trials and/or prospective cohort studies
Study Subjects:
- Reviews that included studies from high or very high human development (2012 Human Development Index)
- Healthy or at elevated chronic disease risk
Intervention/Exposure:
- Low-calorie sweetener - The Committee approached this topic broadly, including sweeteners labeled as low-calorie sweeteners, non-caloric sweeteners, non-nutritive sweeteners, artificial sweeteners, and diet beverages.
Outcome:
- Body weight: Body mass index, body weight, percent body fat, waist circumference, incidence of overweight or obesity
- Type 2 diabetes: Glucose intolerance, insulin resistance, or incidence of type 2 diabetes
Quality:
- Reviews rated 8-11 on AMSTAR (A measurement tool for the ‘assessment of multiple systematic reviews’)
Search Results
Excluded Articles with Reason for Exclusion
- Althuis MD, Weed DL, Frankenfeld CL. Evidence-based mapping of design heterogeneity prior to meta-analysis: a systematic review and evidence synthesis. Syst Rev. 2014;3:80. PMID: 25055879. http://www.ncbi.nlm.nih.gov/pubmed/25055879. EXCLUDE: Discusses design heterogeneity in SSB research; does not address the question
- Bader JD. Casein phosphopeptide-amorphous calcium phosphate shows promise for preventing caries. Evid Based Dent. 2010;11(1):11-2. PMID: 20348890. http://www.ncbi.nlm.nih.gov/pubmed/20348890. EXCLUDE: Does not examine a low-calorie sweetener (CPP-ACP is a milk-derived product that is intended to remineralize teeth)
- Brahmachari G, Mandal LC, Roy R, Mondal S, Brahmachari AK. Stevioside and related compounds - molecules of pharmaceutical promise: a critical overview. Arch Pharm (Weinheim). 2011;344(1):5-19. PMID: 21213347. http://www.ncbi.nlm.nih.gov/pubmed/21213347. EXCLUDE: Narrative review
- Brown RJ, Rother KI. Non-nutritive sweeteners and their role in the gastrointestinal tract. J Clin Endocrinol Metab. 2012;97(8):2597-605. PMID: 22679063. http://www.ncbi.nlm.nih.gov/pubmed/22679063. EXCLUDE: Narrative review
- Cabrera Escobar MA, Veerman JL, Tollman SM, Bertram MY, Hofman KJ. Evidence that a tax on sugar sweetened beverages reduces the obesity rate: a meta-analysis. BMC Public Health. 2013;13:1072. PMID: 24225016. http://www.ncbi.nlm.nih.gov/pubmed/24225016. EXCLUDE: Examined evidence on SSB tax; does not address the question
- Cohen L, Curhan G, Forman J. Association of sweetened beverage intake with incident hypertension. J Gen Intern Med. 2012;27(9):1127-34. PMID: 22539069. http://www.ncbi.nlm.nih.gov/pubmed/22539069. EXCLUDE: Not a systematic review or meta-analysis (prospective analysis to examine associations between SSBs and ASBs with self-reported incident hypertension)
- Daniels MC, Popkin BM. Impact of water intake on energy intake and weight status: a systematic review. Nutr Rev. 2010;68(9):505-21. PMID: 20796216. http://www.ncbi.nlm.nih.gov/pubmed/20796216. EXCLUDE: Out of scope, systematic review of studies evaluating the impact of drinking water compared with no beverage or other beverages on energy intake and/or weight status
- Franz MJ, Powers MA, Leontos C, Holzmeister LA, Kulkarni K, Monk A, et al. The evidence for medical nutrition therapy for type 1 and type 2 diabetes in adults. J Am Diet Assoc. 2010;110(12):1852-89. PMID: 21111095. http://www.ncbi.nlm.nih.gov/pubmed/21111095. EXCLUDE: Describes medical nutrition therapy for type 1 and type 2 diabetes
- Goyal SK, Samsher, Goyal RK. Stevia (Stevia rebaudiana) a bio-sweetener: a review. Int J Food Sci Nutr. 2010;61(1):1-10. PMID: 19961353. http://www.ncbi.nlm.nih.gov/pubmed/19961353. EXCLUDE: Narrative review
- Keukenmeester RS, Slot DE, Putt MS, Van der Weijden GA. The effect of medicated, sugar-free chewing gum on plaque and clinical parameters of gingival inflammation: a systematic review. Int J Dent Hyg. 2014;12(1):2-16. PMID: 23790138. http://www.ncbi.nlm.nih.gov/pubmed/23790138. EXCLUDE: Examined medicated, sugar-free gum (defined as containing antimicrobial agents or herbal extracts)
- Keukenmeester RS, Slot DE, Putt MS, Van der Weijden GA. The effect of sugar-free chewing gum on plaque and clinical parameters of gingival inflammation: a systematic review. Int J Dent Hyg. 2013;11(1):2-14. PMID: 22747775. http://www.ncbi.nlm.nih.gov/pubmed/22747775. EXCLUDE: dental carries not included as outcome; review focused on comparisons with no chewing gum as a control
- La Vecchia C. Low-calorie sweeteners and the risk of preterm delivery: results from two studies and a meta-analysis. J Fam Plann Reprod Health Care. 2013;39(1):12-3. PMID: 23296849. http://www.ncbi.nlm.nih.gov/pubmed/23296849. EXCLUDE: Did not examine CVD, T2D, body weight, or dental caries as an outcome
- Mallikarjun S, Sieburth RM. Aspartame and risk of cancer: A meta-analytic review. Arch Environ Occup Health. 2013. PMID: 24965331. http://www.ncbi.nlm.nih.gov/pubmed/24965331. EXCLUDE: Did not examine CVD, T2D, body weight, or dental caries as an outcome
- Pereira MA. Diet beverages and the risk of obesity, diabetes, and cardiovascular disease: a review of the evidence. Nutr Rev. 2013;71(7):433-40. PMID: 23815142. http://www.ncbi.nlm.nih.gov/pubmed/23815142. EXCLUDE: Narrative review
- Poolsup N, Pongmesa T, Cheunchom C, Rachawat P, Boonsong R. Meta-analysis of the efficacy and safety of stevioside (from stevia rebaudiana bertoni) in blood pressure control in patients with hypertension. Value in Health. 2012;15(7):A630. EXCLUDE: Examines treatment of blood pressure
- Shankar P, Ahuja S, Sriram K. Non-nutritive sweeteners: review and update. Nutrition. 2013;29(11-12):1293-9. PMID: 23845273. http://www.ncbi.nlm.nih.gov/pubmed/23845273. EXCLUDE: Narrative review
- Ulbricht C, Isaac R, Milkin T, Poole EA, Rusie E, Grimes Serrano JM, et al. An evidence-based systematic review of stevia by the Natural Standard Research Collaboration. Cardiovasc Hematol Agents Med Chem. 2010;8(2):113-27. PMID: 20370653. http://www.ncbi.nlm.nih.gov/pubmed/20370653. EXCLUDE: Focused on treatment